




Northern Light
Superstar
Where did you find those? The Ont. Govt. page at https://covid-19.ontario.ca/data still hasn't been updated.
John Michael McGrath's Twitter:
Dr. Jennifer Kwan is also good.
|
|
|
Where did you find those? The Ont. Govt. page at https://covid-19.ontario.ca/data still hasn't been updated.

 ca.reuters.com
ca.reuters.com
It’s been hard to resist starting every post focusing on the MTA’s current ridership situation and budget woes with the sentence, “It’s been a rough few months for transit,” but it’s been a rough few months for transit. Often associated with the hoi polloi and dirty masses, most transit systems didn’t have reputations for cleanliness before the pandemic and whether fairly or not, quickly become associated with the spread of disease as the pandemic descended on the world.
After a spring in which a spurious MIT study that relied heavily on a correlation/causation error drove the conversation, a group of pro-transit researchers are fighting back, and in a new study released by the American Public Transportation Association, they report no known links between coronavirus cases and public transit.
“As of August 2020, no outbreaks have been traced to public transit in the United States,” the report, authored by New York’s own Sam Schwartz, said. “Based on our data review of case rates and transit usage in domestic cities, the correlation between infection rates and transit usage is weak or non-existent.”
Schwartz’s survey of current pandemic experiences is part of a larger report on transit-related best practices for the COVID-19 era, and you can access the report here as a PDF. It’s very much yet another attempt to change the narrative. The MIT study came out early in April, and despite debunking by Alon Levy and Aaron Gordon, two well-respected voices within the transit community, it set the stage for months of American fears over transit.
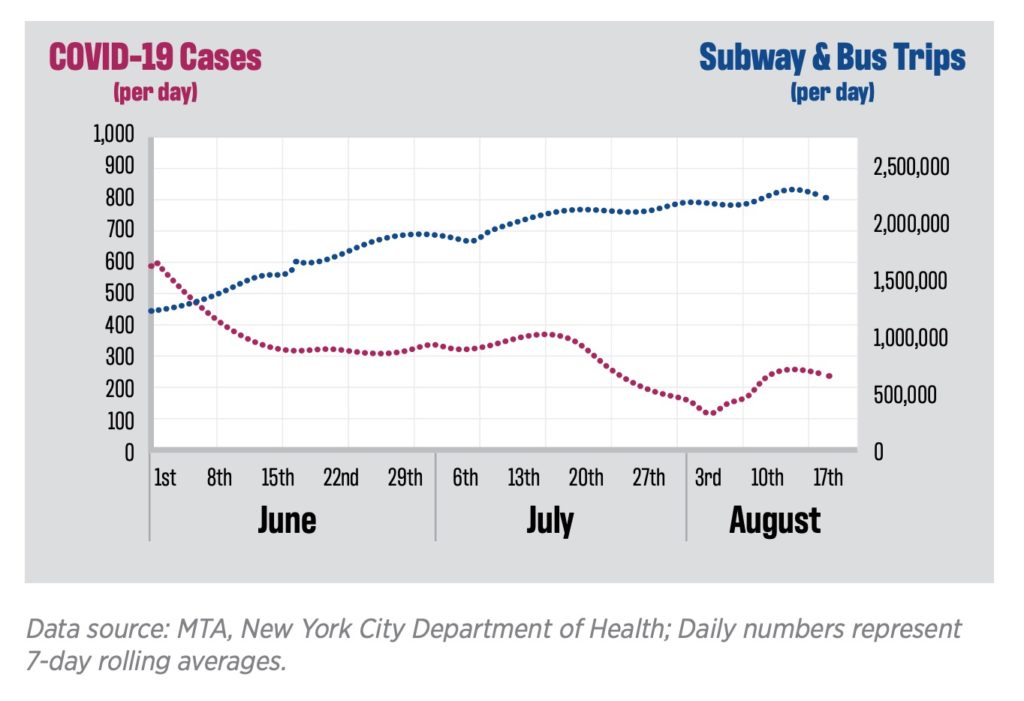
Nearly immediately, many one-time transit riders relied upon the MIT study to reinforce ideas that transit isn’t safe and is a source of spread. Even now, seven months after New York started working from home en masse, subway ridership is only around 1.7-1.8 million per day, approximately 30% of normal, and many New Yorkers have said their commute is the biggest barrier to returning to work. The problem is one of psychology and one of science. I understand why people may be hesitant to ride the subway or hop a bus where they may have less control over everyone around them, but sitting in a poorly ventilated office with other people for 8-10 hours a day is more dangerous than the ride shorter to get there. Schwartz is trying to prove it.
Schwartz has to overcome the challenges of proving a negative, and he makes a compelling case. He looks at transit agencies large and small, from NYC to Hartford to the Quad Cities to Northern Kentucky. In each case, after lockdowns eased, increased transit ridership hasn’t corresponded to an uptick in coronavirus cases. Since the spring at least, when mask mandates were instituted and social distancing became the norm, careful transit usage coupled with disinfectant procedures haven’t led to an uptick in positive tests. Here’s Schwartz’s conclusion:
What Schwartz cannot ascertain and what will always remain unanswered is whether transit had a role in community spread before we had a better understanding of the science behind COVID-19. It’s generally accepted that the virus was in the U.S. long before the middle of March, and 5.5 million people were riding the subways each day well into early March and long before we knew how effective masks were at slowing the spread. Schwartz even admits as much, noting that “public transit has some characteristics associated with higher COVID-19 transmission risk, including the potential for crowding in enclosed environments on trains, buses and indoor stations.” Ultimately, though, masks, a lack of talking, frequent air replacement and a steady flow of passengers mitigates against risks today whether or not the trains helped spread the virus in March. Based on what we know now, so long as most riders are masked, it’s safe to ride transit.
But will this report matter? That is a question I can’t answer. People’s fears about COVID-19 are fairly baked in right now, and while mayoral candidates are making a show of riding trains, neither Bill de Blasio nor Andrew Cuomo have issued full-throated defenses of subways lately. For better or worse, potential transit riders take their cues from leadership, and leadership is wavering. Still, Schwartz’s study and overview reinforces what many of us have been saying: With proper precautions and a smart approach to personal and communal care, transit trips are no more riskier than any other activity these days.
The final wild card in this psychological battle for the minds of transit riders is, of course, the Trump Administration. Hardly allies to cities and transit riders, the White House has blocked a national order requiring face masks on all transit hubs. Instead, it’s up to localities to approve and enforce these orders. At a local level, the MTA is also prohibited from applying for a federal grant to study how to combat coronavirus spread on transit, as Politico reported late last week.
We’ll know more about this development on Monday, but this is the heigh of petty politics. Despite its flaws, the MTA is best suited to understand how to combat COVID on transit, and the fact that they can’t apply for this grant because the Trump Administration is playing politics with public health three weeks before the election is a travesty. Still, we know the answers — masks, constant service, less talking, ventilation and high-quality air filters. That’s how transit is safe, and that’s why you could ride the subways today without worrying too much about putting your health at risk.
Is COVID increasing income inequality? https://www.ctvnews.ca/business/ric...42835#_gus&_gucid=&_gup=Facebook&_gsc=8MHC4Bm
I'm thinking about the ladies at the Scotia Plaza food court. They don't conform to the stereotype of a young student on their way to a "better job".I would not for one second doubt it. Women/casual workers in low-paying service sectors are the ones getting hit the hardest by the pandemic.
AoD
The lockdown in Australia is cause there is no widespread community spread in Australia as it is an island.
We are not in that stage and even with harsh lockdown for months, we will have cases coming from travel and from the USA forcing us into non-stop lockdowns of Toronto and our major cities over a few cases. It would be an unsustainable situation for the country.
So the Australian model is not a valid model for Canada at all.
plus Canadians are not as supportive of harsh measures.
Why dont you guys understand that?
There are tens of thousands that cross the US border daily for work including medical workers, but also truck drivers.And, seriously, you need to drop the whole Canada is not an island thing - as I asked in this thread before, you can't just waltz into Canada whenever you like at which ever point you like, correct? People go through checkpoints, on the land, at airports or sea ports - you can effectively "island" yourselves like we have with our permanent moat.
Likewise, how do you think covid got to Canada? Likely by an infectious person who arrived by air.
There's a daily media release with detailed data on our cases, latest version is here: https://www.dhhs.vic.gov.au/coronavirus-update-victoria-15-october-2020
There are tens of thousands that cross the US border daily for work including medical workers, but also truck drivers.
I'm not arguing that it is responsible for most transmission, but that Canada has a structurally different flow of people across the border when compared to Australia. And if we ever got Canada down to such a low level of community spread as Australia is seeing, then cross-border transmission would be an on-going source of infection. So, it is kind of hopeless to try to achieve that level of suppression. Honestly, I'm not even sure it is desirable. It might be better to have the virus continue to work its way through the population at a modest, manageable rate to continue to build herd immunity.