Hmmm, how about we look at hard science, as opposed to conjecture.
Here's a study of the effectiveness of different measures world wide in controlling the spread of Covid.
Note the limitations, there are different ways to analyze the data this study used 4, and shows you the results for all 4, which sometimes conflict.
Seeing which measure produce meaningful improvements under all types of analysis (and which demonstrably fail is interesting)}
Also the data does not examine secondary negative effects such as delayed medical treatments, economic or mental health harm. Its simply a hard look at what at least does what it says it sets out to do; reduce spread.
Analysing over 50,000 government interventions in more than 200 countries, Haug et al. find that combinations of softer measures, such as risk communication or those increasing healthcare capacity, can be almost as effective as disruptive lockdowns.

www.nature.com
From said study, the charts aforementioned:
View attachment 293748
Explanation to read the above:
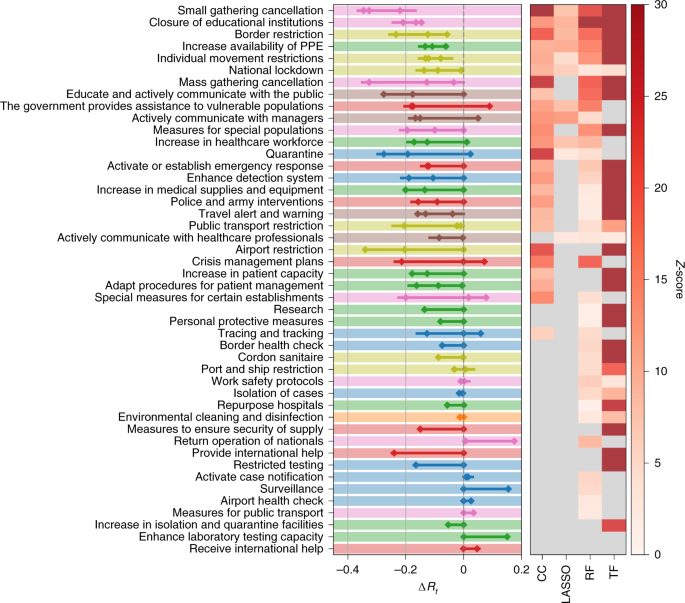
The left-hand panel shows the combined 95% confidence intervals of ΔRt for the most effective interventions across all included territories. The heatmap in the right-hand panel shows the corresponding Z-scores of measure effectiveness as determined by the four different methods. Grey indicates no significantly positive effect. NPIs are ranked according to the number of methods agreeing on their impacts, from top (significant in all methods) to bottom (ineffective in all analyses). L1 themes are colour-coded as in Supplementary Fig. 1.
Study conclusions:
Among the six full-consensus NPI categories in the CCCSL, the largest impacts on Rt are shown by small gathering cancellations (83%, ΔRt between −0.22 and –0.35), the closure of educational institutions (73%, and estimates for ΔRt ranging from −0.15 to −0.21) and border restrictions (56%, ΔRt between −0.057 and –0.23).
The consensus measures also include NPIs aiming to increase healthcare and public health capacities (increased availability of personal protective equipment (PPE): 51%, ΔRt −0.062 to −0.13), individual movement restrictions (42%, ΔRt −0.08 to −0.13) and national lockdown (including stay-at-home order in US states) (25%, ΔRt −0.008 to −0.14).
Note that lock down produces the lowest positive score among 'effective measures'.
The Least effective measures were:
Among the least effective interventions we find: government actions to provide or receive international help, measures to enhance testing capacity or improve case detection strategy (which can be expected to lead to a short-term rise in cases), tracing and tracking measures as well as land border and airport health checks and environmental cleaning.
************
This is really useful, scientific information.
I have concluded reading the abstract but want to drill down into some of the details which also matter greatly.





")